
AMH 0.8: Can You Still Get Pregnant Naturally or Through IVF? What Your Report Really Means
There is a particular kind of silence that follows an AMH report.
The doctor circles a number. You reach home and type it into Google. Within minutes, you are reading words like low ovarian reserve, poor response, and sometimes even diminished fertility. By the time you have finished scrolling, it feels as though one laboratory value has already decided your future.
It hasn't.
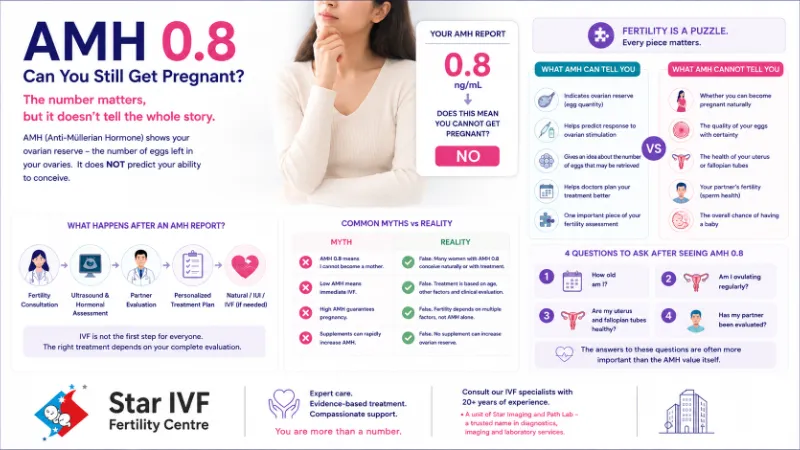
An AMH value of 0.8 ng/mL deserves attention, but it does not deserve panic. It is a biological marker, not a verdict. In fertility medicine, numbers only become meaningful when they are interpreted alongside age, ultrasound findings, menstrual history, and the overall health of both partners.
Perhaps the biggest misconception surrounding AMH is that it measures the ability to become pregnant. It does not. It primarily reflects ovarian reserve, or the estimated number of eggs remaining in the ovaries. Quantity, however, is only one part of a much larger equation.
A woman may have a modest ovarian reserve and still conceive naturally. Another may have a reassuring AMH level yet struggle because of factors unrelated to ovarian reserve. Fertility has never been a single-number science, despite what social media often suggests.
Why does AMH receive so much attention?
Because it helps doctors plan.
When fertility specialists evaluate a patient, they are trying to understand how the ovaries are likely to respond and what strategy would offer the best chance of success. AMH becomes one piece of that assessment. It guides decision-making, but it does not make decisions on its own.
Think of it this way: a fuel gauge tells you how much fuel is available, but it cannot predict the entire journey. The condition of the engine, the route, the driver, and the destination all matter.
The same principle applies to fertility.
The question patients actually want answered
The search query is usually:
"My AMH is 0.8. Can I still get pregnant?"
The honest answer is yes, it is possible.
But honesty also requires acknowledging that every case is different. Age plays a significant role. Ovulation patterns matter. The condition of the uterus and fallopian tubes matters. Equally important is the male partner's fertility, a factor that is often underestimated despite contributing to a substantial proportion of infertility cases.
This is precisely why experienced fertility specialists rarely react to an AMH report in isolation. They build a clinical picture before recommending a treatment pathway.
One report should never become your identity
Many women begin introducing themselves to doctors by saying,
"I have low AMH."
In reality, they have a laboratory report indicating a particular ovarian reserve. That report should inform medical discussions, not define them.
Medicine is full of examples where clinical outcomes differ from expectations. Fertility is no exception. There are women with seemingly reassuring reports who require advanced treatment, and there are women with lower AMH values who achieve pregnancy with comparatively simple interventions.
The difference lies in comprehensive evaluation rather than assumptions.
What happens after a low AMH report?
This is where expertise matters.
A fertility consultation should answer questions that a laboratory report cannot.
- How many follicles are visible on ultrasound?
- Are menstrual cycles regular?
- Is ovulation occurring consistently?
- Is there evidence of endometriosis or other gynecological conditions?
- Has the male partner undergone a semen analysis?
- Would trying naturally still be reasonable, or would assisted reproductive techniques improve the chances?
These are medical decisions that require interpretation rather than internet speculation.
At Star IVF Fertility Centre, consultations are designed around this broader understanding of fertility. Patients are evaluated by IVF specialists with more than two decades of experience, while also benefiting from the strong diagnostic and imaging foundation of Star Imaging and Path Lab, an institution that has served patients across diagnostics, imaging, and laboratory medicine for decades. The objective is straightforward: understand the complete clinical picture before discussing treatment options.
Does low AMH automatically mean IVF?
No.
One of the most persistent myths is that a reduced AMH level immediately leads to IVF. That is simply not how responsible fertility medicine works.
Some couples may be advised to continue trying naturally for an appropriate period. Others may benefit from ovulation monitoring or medical management. Some may be suitable candidates for IUI, while others may indeed require IVF depending on age, ovarian reserve, duration of infertility, and additional clinical findings.
The recommendation should emerge from evidence, not fear.
Why comparing reports with others can be misleading
Online forums are filled with statements such as,
"My AMH was 0.6 and I conceived naturally."
or
"My AMH was 3.5 and IVF still failed."
Both stories may be true.
They are also clinically incomplete.
No two patients share the exact same reproductive profile. Comparing laboratory values without considering age, embryo quality, uterine factors, and male fertility is like comparing two books after reading only the title.
Your fertility journey deserves a more individualized assessment.
The conversation that should replace panic
Instead of asking,
"Is my AMH too low?" consider asking,
"Given my age and overall fertility profile, what is the most appropriate next step?"
That shift in perspective changes the discussion from anxiety to planning. And planning is where modern reproductive medicine is at its strongest.
The takeaway
An AMH value of 0.8 ng/mL should encourage informed medical evaluation, not hopelessness. It is a useful clinical marker, but it is only one chapter of a much larger story.
The couples who make the best decisions are rarely those who spend weeks collecting opinions online. They are the ones who seek a thoughtful assessment, understand their options, and move forward with clarity.
Because in fertility medicine, the most important number is not always the one printed on the report. It is the one that reflects the opportunity created by timely and expert guidance.




